Dental caries (commonly referred to as cavities), periodontal disease, and tooth loss now affect more than 45% of the world’s population, with about 3.5 billion people living with untreated oral diseases; this surpasses numbers for any other non-transmissible disease. Cases of oral diseases have grown by 1 billion during the past 30 years. Dental caries alone is the most prevalent health condition, while periodontitis is the eleventh most prevalent – both having a significant impact on overall health and quality of life. The prevalence of these oral diseases is notably influenced by health inequalities, with 3 out of 4 people affected by these oral diseases living in low- and middle-income countries, as existing therapies ultimately require professional intervention and access to dental care, which are significantly reduced in resource-limited populations. As a result, there remains significant need for alternative approaches to manage these oral diseases, including prevention of the disease, regeneration of compromised tissues, and reconstruction of lost tissues and function.
Dental caries
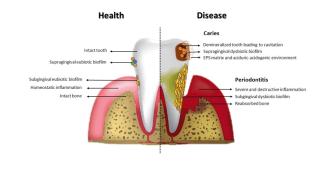
The microbial communities on the tooth surface remain stable if there is a low frequency sugar intake. Although they are able to produce acids that demineralize enamel, the intermittent pH decrease can be neutralized by saliva, which restores and maintains the mineralization of enamel. However, with frequent exposure to fermentable carbohydrates, microorganisms become embedded in a biofilm matrix rich in extracellular polymeric substances (EPS) while constantly producing acids. If the cariogenic (cavity-causing) biofilm is not removed and frequent sugar consumption continues, a prolonged and repeated state of acidification ensues, disrupting the homeostatic mineral balance towards enamel demineralization. The dysbiotic microorganisms interact with each other in a dynamic and concerted polymicrobial synergy which changes as caries progress from early onset (initial demineralization) to deeper lesions with dentin exposure. Therefore, dental caries can be described as a multifactorial disease associated with overexposure to dietary carbohydrates. Host factors and accumulation of acidogenic (acid-producing) and aciduric (acid-tolerant) microorganisms further promote the production of acidic metabolites and EPS that cause the destruction of the mineralized tooth tissue and cavitation.
When the dental microbial biofilm builds up on tooth surface, it can also start a direct immune response resulting in an inflammatory condition of the soft tissues surrounding the teeth (gingiva). This condition, designated gingivitis, can be altered by several factors such as smoking, certain drugs and hormonal changes (e.g. puberty and pregnancy). If the gingivitis progresses, the inflammatory condition also affects the surrounding supportive structures and periodontitis can be established, involving the destruction of the periodontal ligament, bone and soft tissues – which eventually leads to tooth loss. Although this disease is initiated by a dysbiotic biofilm it only occurs in a subgroup of the population, as it is influenced by the virulence of the oral microbiome and the individual’s immune and inflammatory responses.
References
Benzian H, Watt R, Makino Y, Stauf N, Varenne B. WHO calls to end the global crisis of oral health. Lancet. 2022;400(10367):1909-1910. doi:10.1016/S0140-6736(22)02322-4
Lamont RJ, Koo H, Hajishengallis G. The oral microbiota: dynamic communities and host interactions. Nat Rev Microbiol. 2018;16(12):745-759. doi:10.1038/s41579-018-0089-x
Kinane DF. Causation and pathogenesis of periodontal disease. Periodontol 2000. 2001;25:8-20. doi:10.1034/j.1600-0757.2001.22250102.